The Preceptor's Choice
A branching-video experience that teaches clinical preceptors to recognize everyday incivility — by letting them feel where their choices land on a student.
The Problem
"Nurses eat their young."
The Nursing department came to my team with a painful, specific problem. Their students were reporting genuinely poor experiences under the preceptors entrusted with training them — not being treated with dignity, not having the clinical work explained to them, and being verbally or publicly shamed when they made mistakes. It has a grim nickname in the field: "nurses eat their young." They wanted an immersive, innovative learning experience that could begin to change that culture.
What makes this a hard design problem, and not just a hard people problem, is the audience. Incivility training almost always fails for the same reason: nobody believes they're the uncivil one. Tell a room of preceptors to be kinder and every one of them will nod along, certain the message is meant for someone else. You cannot lecture a person out of a behavior they don't think they have.
You can't tell preceptors to be kinder — every one of them thinks they already are. You have to let them watch their own choice land on someone.
The Insight
Put them in the seat. Show them the consequence.
I designed the experience — and wrote every scenario — around a single principle: don't describe the behavior, let the learner perform it and feel the result. The preceptor completing the experience is the preceptor in the story. At each turning point, they make a real decision, and then they watch it land on the student, whose confidence visibly builds or quietly erodes depending on what they chose.
The crucial design choice is that no option is a cartoon villain. The decisions hinge on the exact tension every preceptor actually lives inside: the pressure of the task and the clock versus the time it takes to bring a student in. Nobody chooses to be cruel. They choose to protect the schedule — and the experience shows them, without judgment, what that costs. That subtlety is the whole thing. Preceptors have to recognize themselves in the choice, or the lesson never lands.
How it works
A decision with no obvious right answer.
The learner moves through a clinical shift as short video vignettes. At each choice point, they're handed a realistic dilemma with a few plausible responses — and the branch they pick changes what happens next.
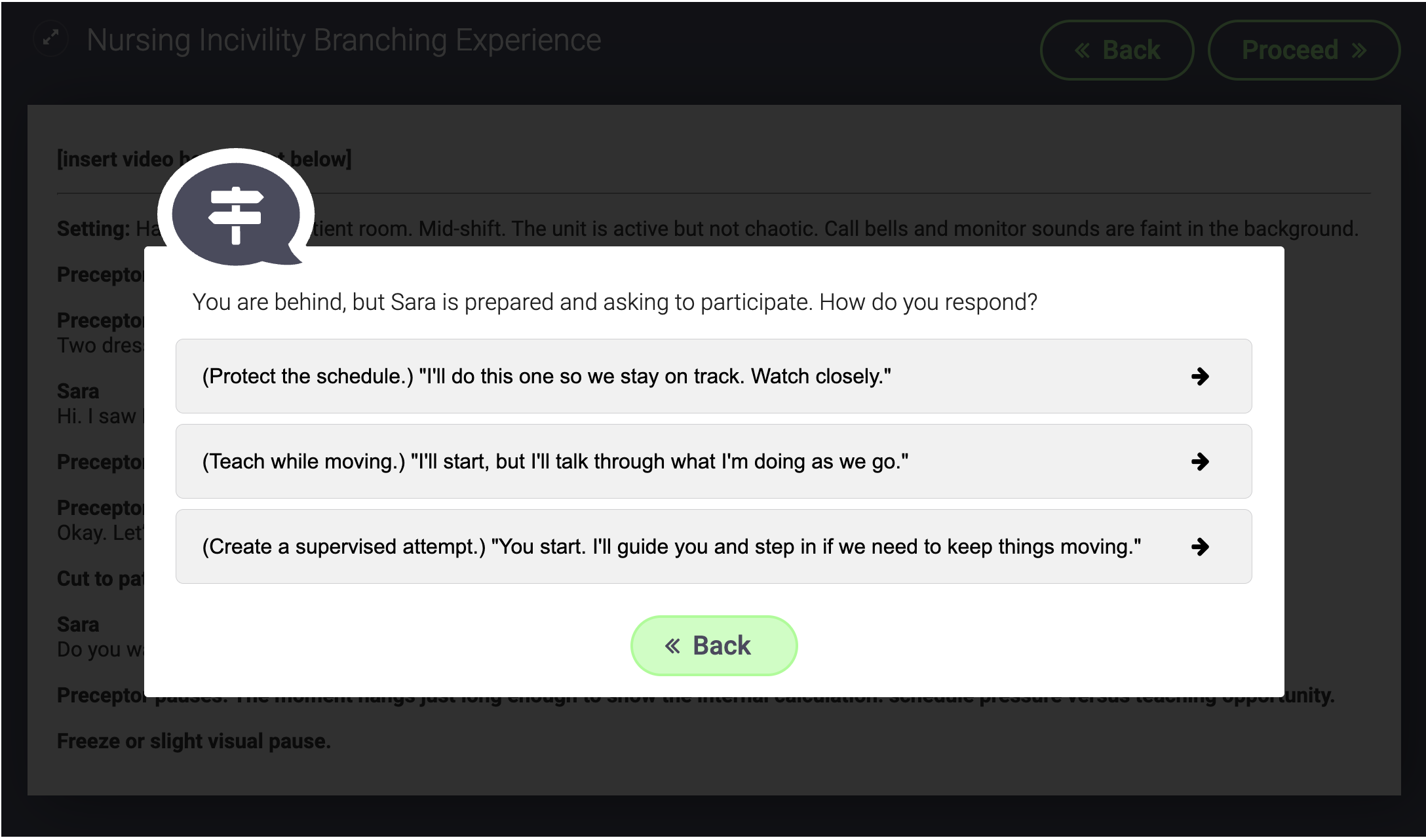
In an early scenario, the preceptor is changing a patient's dressings while running behind. The options are the same three every preceptor weighs in real life: do it yourself while the student watches, do it yourself but slow down and narrate each step, or let the student do it with feedback along the way. None is wrong on paper. But each one sends a different signal to the student about whether they're a burden or a participant — and those signals accumulate.
A scene, up close
The same heartbeat, two different endings.
Here is where the design earns its keep. In Scenario 2, the student — Sara — has gone quiet all morning. The preceptor notices in the hallway, and the learner is asked to choose:
Sara has been quieter than usual today. What do you do?
Moments later, in every branch, the scene arrives at the same clinical fact: the patient's heart rate has been sitting in the low 50s, and a medication is about to be given. What changes is whether Sara feels safe enough to say so.
If you protect the task (a)
Sara watches the vitals. Her eyes pause on the heart rate. She looks like she is considering asking something, but she does not.
The medication is scanned. Sara stays quiet. The moment passes — and so does the catch.
If you make space (b / c)
Sara exhales. "His heart rate was 58 earlier. Is that okay with this medication?"
The preceptor stops. "Good catch. Let's double-check the parameters." A silent student would not have said it.
That is the argument the whole experience is built to make, and it makes it without a single line of lecture: incivility isn't only unkind. A student who doesn't feel safe to speak is a student who won't flag the thing that matters — and in a hospital, the thing that matters is sometimes a patient's life. The design connects a small, forgettable moment of warmth to a genuine safety outcome, and lets the preceptor discover that link themselves.
The production
Built across departments.
This is a cross-functional production. The concept, the branching structure, and every scenario script are mine; the experience is built and branching in H5P. For the vignettes, we're partnering with FIU's Theatre department to cast students in the roles — deliberately, both to get real performances of these subtle nonverbal moments and to grow the kind of inter-departmental collaboration these projects are meant to model. The nonverbal beats are where the whole design lives, which is exactly why trained actors matter.
Where it stands
Honest status: in development.
To be clear about what's done and what isn't: the five scenarios are scripted, and the branching experience is fully built in H5P. What remains is filming the vignettes on campus with the Theatre students, editing, and dropping them into the branches — and then it launches. There's no learner data yet, and I won't imply otherwise.
What I can point to is the response from the people who know this problem best. The Nursing team has been enthusiastic about the scenarios specifically because they're not only compelling but realistic — true to situations preceptors actually find themselves in, which is the hardest bar to clear when you're writing for a clinical audience. That credibility, from the subject-matter experts, is the signal I'd trust most at this stage.
Why it works
The theory under the design.
The core mechanism is psychological safety — the well-documented finding that people only speak up about risks when they feel safe to do so, and that in clinical settings the willingness to speak up is directly tied to catching errors. The experience doesn't teach that concept; it stages it, so a preceptor watches their own behavior open or close that channel in a student. It leans on consequence-based, situated learning: we retain what we experience the results of far better than what we're told, so every choice produces a visible outcome rather than a score. And the branching structure is doing real work — by letting preceptors take the "protect the task" path and live its cost in a safe simulation, it lets them make the mistake where no patient is harmed, which is the entire point of scenario-based training.
The restraint is deliberate, too. Nothing moralizes. The design trusts that if you build the moment accurately enough, the preceptor will draw the conclusion themselves — and a conclusion you reach on your own is one you actually keep.
The bigger idea
Changing the mind of someone who thinks they're already right.
This is my behavior-change artifact, and behavior change in a resistant audience is one of the hardest problems in all of communication — which is precisely why it transfers. The preceptors here are exactly the audience a lot of content and messaging work has to move: people who don't think the message applies to them. The winning move isn't a stronger argument. It's an experience that lets them arrive at the realization on their own, because a belief someone reaches themselves is the only kind that changes behavior. That's true whether you're shifting a clinical culture or a customer's mind.
The rest is content-craft I'd bring to any team: designing genuinely interactive, choice-driven content rather than passive information; writing for emotional resonance over information transfer, so an audience feels a consequence instead of reading a policy; and producing it across functions — briefing and partnering with a separate creative team (here, Theatre) to get the performance the concept needs. Different subject, same discipline: understand the audience precisely enough to build the one experience that moves them.